Where does Kinesiology come from?
Muscle testing was first used in the early 20th century to measure muscle weakness in polio victims. In 1949 Kendall and Kendall, two physiotherapists had developed specific ways to test individual muscles for other neuromusculoskeletal conditions.
By 1964, Chiropractor Dr George Goodheart DC developed Applied Kinesiology based on Kendall and Kendall’s technique. Dr Goodheart’s technique not only evaluated muscle power but also evaluated how well the nervous system controlled muscle function.
Dr Goodheart went on to combine his knowledge of chiropractic techniques, neuro-lymphatic reflexes, nutrition and Traditional Chinese Medicine to further develop Applied Kinesiology. Applied Kinesiology was aimed specifically at professional healthcare practitioners. In the U.K, Applied Kinesiology is known as Systematic Kinesiology.
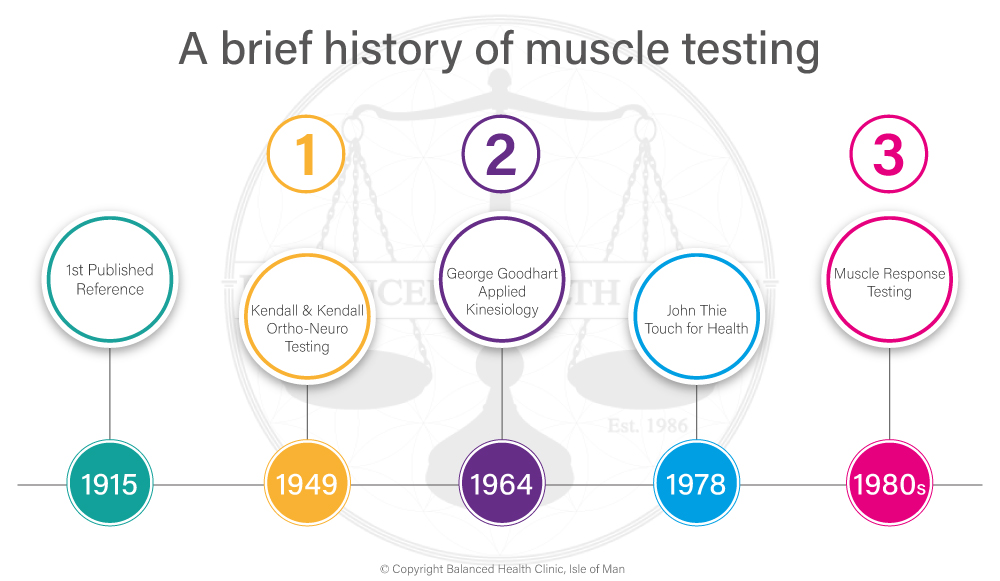
In 1978, Kinesiology was adapted by John F Thie, who developed Touch for Health Kinesiology, making it accessible to the non-professional public.
Dr George Goodheart DC and the creation of Applied Kinesiology
Applied Kinesiology was originally developed by Dr George Goodheart DC., a second generation chiropractor, in the early 1960’s. He discovered the relationship between Chinese meridians (used by practitioners of Chinese medicine including acupuncturists) and muscle groups, organs, and glands in the body. By testing the resistance of a muscle when a small amount of pressure is applied to it, weaknesses and imbalances in its corresponding meridian could be distinguished. The technique was developed into the system of Kinesiology known as Applied Kinesiology that was used mostly by medical related practitioners such as dentists and chiropractors.
In Dr George Goodheart’s own words,
“Applied Kinesiology had a simple beginning in 1964, based on the conceptthat antagonist
muscle weakness is involved in most muscle spasms and, indeed, is primary.”
(ref: Walther, 1988).
Basically, Dr Goodheart’s discovery of Applied Kinesiology started out of his observation that basic Chiropractic adjustments often were not providing complete relief for physical disabilities and that the problem seemed to be related to muscle spasms that were not being released. In 1949 a study by Kendall and Kendall looked into the original methods of testing muscles which led to the main diagnostic tool of muscle testing that is now used in Applied Kinesiology. Dr Goodman, together with his colleague Dr Alan Beardall DC changed the timing of the muscle testing procedure to provide an assessment of the control of the muscle by the nervous system, rather than an assessment of the power that the muscle could produce.
Dr Goodheart observed that inhibited muscles often displayed none of the visible deterioration that he expected to find in a physically malfunctioning muscle. He also observed, through palpation, discrete painful nodules at the muscle insertion. Wondering if these nodules might be trigger points for the muscle, he deeply massaged these nodules and found that the muscle immediately regained a high percentage of its strength and that the nodules became less painful. (ref: Goodheart, 1964)
By continually asking “why is that?” Dr Goodheart has found the answers to many health questions. Dr Goodheart’s observations have been annually published since 1964. As the result of Dr. Goodheart’s sharing the knowledge in applied kinesiology has snowballed with contributions from students of Dr. Goodheart.

- Kinesiology uses simple muscle testing procedures to find problem areas, and uses massage, touch, nutrition, and counselling to balance holistically.
- Kinesiology is a natural health care system, which uses gentle muscle testing to evaluate many functions of the body in the structural, chemical, neurological, and biochemical realms.
- Kinesiology testing does not diagnose disease. Muscle testing enables analysis, which detects minor functional imbalances. Minor imbalances when not corrected, accumulate and cause compensations.
- Using massage, nutrition, and contact points, Kinesiology helps with: emotions and anxieties, specific personal dietary intake and supplements for nutritional deficiencies, structural imbalances and energy blocks. Kinesiology balances the whole person, which enhances health and well-being. Health wards off disease. Kinesiology is truly preventive.
- There is research on applied kinesiology. There are numerous studies in the medical literature on the manual muscle testing methods that are the basis of applied kinesiology. These include:
- A study which showed significant differences in cortical activity during the applied kinesiology testing of facilitated muscles versus inhibited muscles (Leisman, 1989, International Journal of Neuroscience)
- A study showing significant, reproducible differences between facilitated versus inhibited muscles through needle EMG (Leisman, 1995, Perceptual and Motor Skills)A study showing interexaminer reliability of manual muscle testing for individual muscles (Lawson, 1997, Perceptual and Motor Skills)
- A repetition of the interexaminer reliability study (Perceptual and Motor Skills, in press)
- A study currently in press in the Journal of Manual and Manipulative Therapy demonstrating resolution of a herniated disc with applied kinesiology methods, shown with pre- and post-MRI.
- Manual muscle testing is a standard part of neurologic examinations performed by chiropractors and medical doctors. Muscle testing and reflex responses are the way neurologists assess neurologic motor function.
- Applied kinesiology is nothing more than an extension of the basic neurologic exam. Neurologists and applied kinesiologists both introduce sensory stimuli of known value in pathways whose anatomy is known, and observe expected changes in motor function.
- There are, however, some who have taken this basic observational method beyond the point of science. Observing changes in motor function in response to sensory receptor stimulus is an established scientific practice. The status statement of the International College of Applied Kinesiology states clearly that applied kinesiology is to be practised in addition to other standard forms of diagnosis. One cannot make a diagnosis solely on the basis of manual muscle testing outcomes, though these outcomes can contribute to an overall clinical impression. This is true for any single diagnostic method. Changes in motor function observed via manual muscle testing must be properly interpreted, according to the doctor’s knowledge of neurology, biochemistry, and other relevant diagnostic factors.